
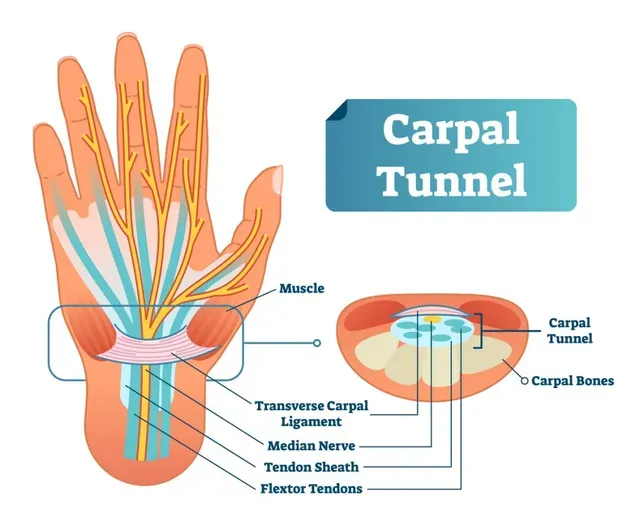
The carpal tunnel is a small space between the wrist (carpal) bones and the transverse carpal ligament, containing nine total muscle tendons, and a nerve called the median nerve (see photo below). Carpal tunnel syndrome (CTS) is caused by an increase of pressure in the carpal tunnel which leads to compression of the median nerve. According to the U.S. Bureau of Labor and Statistics, more than eight million people are affected by carpal tunnel syndrome annually, and it is the most common peripheral nerve entrapment syndrome. Some risk factors for carpal tunnel syndrome include: previous wrist fracture, pregnancy, genetics, repetitive hand use, diabetes, and arthritis (4, 10).
Symptoms are often described as pain, numbness, and/or tingling of the thumb, index finger, middle finger, and half of the ringer finger. Pain may progress to an electric shock like impulse through the affected area. There may also be weakness, clumsiness, and muscle atrophy. Patients typically describe an increase of symptoms when gripping an object such as a phone or steering wheel, and symptoms decrease when shaking or flicking their hand (1, 11).
Healthcare providers must be sure to properly diagnose CTS. Other conditions could be misdiagnosed as CTS, such as cervical radiculopathy, pronator teres syndrome, and anterior interosseous nerve syndrome for example. Physicians may recommend an MRI, ultrasound, electromyography, or nerve conduction studies in order to rule in or rule out CTS.
While carpal tunnel surgery is the second most common musculoskeletal surgery in the USA, other treatment options should be first attempted. Conservative treatments include physical therapy, splinting, local steroid injection, ultrasound, oral steroids, nonsteroidal anti-inflammatory drugs, and vitamin B6 supplementation (6, 9). Due to the increased risk of tendon rupture or median nerve injury, local steroid injections should only be considered after attempting other conservative treatment measures (1). Surgery should be considered if conservative treatment fails, or in the case of severe median nerve damage (8, 11).
Manual physical therapy treatment has been shown to be more effective than surgery in the short-term, and as effective as surgery in the medium-term and long-term at one year follow-up (3). Physical therapy treatments should include education, activity modification, soft tissue mobilization, transverse ligament stretching, carpal bone mobilizations, cervical spine mobilizations, tendon gliding, nerve gliding, and electro-acupuncture (also known as electrical dry needling).
Peri-neural electrical dry needling improves microcirculation and was shown to decrease pain more than night splinting in patients with CTS (2, 7). Dry needling was shown to be more effective than ibuprofen for improving function and improving pain level (5). Furthermore, dry needling was as effective as steroid injections for decreasing pain, numbness, tingling, and weakness, and dry needling was more effective than steroid injections to decrease nocturnal awakening due to CTS (12). Due to the limited risk of dry needling, and the remarkable benefits, dry needling should be used in addition to traditional conservative treatment techniques.
There is undeniable benefit with surgery and steroid injection in the treatment of carpal tunnel syndrome, however, less invasive treatment methods, such as physical therapy, should be performed initially. As discussed, physical therapy has similar, if not better results in the treatment of carpal tunnel syndrome with minimal associated risk.
Author: PT, DPT, Cert. DN Dr. Osama Imam
References
1. Ashworth NL, MBChB. Carpal Tunnel Syndrome Clinical Presentation [Internet]. 1994 [Updated 2014 Aug 25; cited 2015 March 20]. //emedicine.medscape.com/article/327330-clinical.
2. Dunning J, Butts R, Mourad F, Young I, Flannagan S, Perreault T. Dry needling: a literature review with implications for clinical practice guidelines. Phys Ther Rev. 2014;19(4):252-265. doi:10.1179/108331913X13844245102034
3. Fernández-de-Las Peñas C, Ortega-Santiago R, de la Llave-Rincón AI, Martínez-Perez A, Fahandezh-Saddi Díaz H, Martínez-Martín J, Pareja JA, Cuadrado-Pérez ML. Manual Physical Therapy Versus Surgery for Carpal Tunnel Syndrome: A Randomized Parallel-Group Trial. J Pain. 2015 Nov;16(11):1087-94. doi: 10.1016/j.jpain.2015.07.012. Epub 2015 Aug 15. PMID: 26281946.
4. Geoghegan JM, Clark DI, Bainbridge LC, Smith C, Hubbard R. Risk Factors in Carpal Tunnel Syndrome. Journal of Hand Surgery. 2004;29(4):315-320.
5. Hadianfard M, Bazrafshan E, Momeninejad H, Jahani N. Efficacies of Acupuncture and Anti-inflammatory Treatment for Carpal Tunnel Syndrome. J Acupunct Meridian Stud. 2015 Oct;8(5):229-35. doi: 10.1016/j.jams.2014.11.005. Epub 2014 Nov 29. PMID: 26433799.
6. Huisstede BM, Hoogvliet P, Randsdorp MS, Glerum S, van Middelknoop M, Koes BW. Carpal Tunnel Syndrome. Part I: Effectiveness of Nonsurgical Treatments–A Systematic Review. Archives of physical medicine and rehabilitation. 2010 Jul; 91(7):981-1004.
7. Kumnerddee W, Kaewtong A. Efficacy of acupuncture versus night splinting for carpal tunnel syndrome: a rando-mized clinical trial. J Med Assoc Thai. 2010;93(12):1463–9.
8. Khosrawi S, Moghtaderi A, Haghighat S. Acupuncture in treatment of carpal tunnel syndrome: A randomized controlled trial study. J Res Med Sci. 2012;17(1):1-7.
9. O’Connor D, Marshall SC, Massy-Westropp N, Pitt V. Non-surgical treatment (other than steroid injection) for carpal tunnel syndrome (Review). The Cochrane database of systematic reviews. 2012; volume (7):1-106.
10. Stevens JC, Beard CM, O’Fallon WM, Kurland LT. Conditions associated with carpal tunnel syndrome. Mayo Clin Proc. 1992 Jun;67(6):541-8. doi: 10.1016/s0025-6196(12)60461-3. PMID: 1434881.
11. Wipperman J, Goerl K. Carpal Tunnel Syndrome: Diagnosis and Management. Am Fam Physician. 2016 Dec 15;94(12):993-999. PMID: 28075090.
12. Yang CP, Hsieh CL, Wang NH, Li TC, Hwang KL, Yu SC, Chang MH. Acupuncture in patients with carpal tunnel syndrome: A randomized controlled trial. Clin J Pain. 2009 May;25(4):327-33. doi: 10.1097/AJP.0b013e318190511c. PMID: 19590482.
Image obtained from Mayo Clinic.